

I’ll admit where I started, because it’s embarrassing. I typed “is Peptide Sciences legit” into a search bar like everyone else, expecting a tidy yes or no. What I got instead was a stack of affiliate posts, all answering a question nobody asked them: did the site ship on time, did the packaging look nice. Not one of them touched the thing that actually mattered to me, which was whether a licensed human being with a medical degree stood anywhere between me and whatever was in that vial. So I threw out the question and asked a better one. Not “was the old vendor legit,” but “of the telehealth outfits that popped up to replace it, which ones actually have a real physician doing real work behind the curtain?” Here’s the record, such as it is.
The fair version of the old story
Credit where it’s due. Peptide Sciences ran for years as a research-chemical retailer, it shipped what people paid for, and I could not find a verified FDA warning letter against it anywhere in the public record. It’s widely reported to have voluntarily shut down around March 2026 [C1], though I want to be honest that I couldn’t pin that down against any government source, so I’m treating it as a rumor with legs rather than a documented fact. It wasn’t a scam in the classic sense of the word. Nobody vanished with anyone’s money that I could find.
But “was the business real” and “was anyone medically accountable for what you’d be injecting” turned out to be two completely different questions, and once I separated them, the second one had the same flat answer for Peptide Sciences as for every other research-chemical seller I looked at: no. Nobody was.
“Telehealth” is a word, not a promise
Here’s what surprised me first. I figured that once I moved past the obvious research-chemical sites and into anything branded “telehealth,” I’d automatically be somewhere safer. Wrong. Telehealth is a costume you can put on almost any checkout page. A stethoscope icon and an “our physicians” tab don’t tell you anything by themselves.
So I built a cruder test, and it did more work than any star rating I read. Forget whether a site mentions a doctor. Ask instead: would a real clinician actually stop me if this were a bad idea for me? That’s it. That’s the whole test.
Chasing that question down, I landed on four things that are easy to claim and hard to fake:
A genuine intake that can say no. Not a form that waves everyone through, but a real history reviewed by a licensed clinician, with an actual path to “this isn’t right for you.” A screen that approves everybody isn’t screening. It’s set dressing.
A real prescription, written by that clinician. This is the line. If access dead-ends at checkout with nothing written by anyone with a license, no amount of branding changes what you’re buying.
A licensed compounding pharmacy doing the actual dispensing. Under sections 503A and 503B of federal drug law, licensed pharmacies and physicians can compound from a valid prescription, under specific conditions. That’s a regulated chain with named, accountable parties in it. A “lab” mailing a vial is not that chain, no matter what the label says.
Follow-up that actually happens. Monitoring, dose adjustment, someone to call after the first shipment. Safe use of anything is a relationship, not a single transaction.
Once I had that checklist, most of the field sorted itself without much help from me.
Why this stopped being an academic exercise
Part of why this question got urgent wasn’t just the reported Peptide Sciences closure, though that was the trigger. Industry write-ups describe a short notice in early March 2026 announcing the company had “voluntarily decided to shut down operations and discontinue the sale of all research products,” with support lines going quiet and orders reportedly left unfilled [C1]. Again, that’s reported by analysts and affiliate sites, not confirmed by a government filing, and I want to keep saying so because it matters. The one thing every source agreed on: if a site is using the Peptide Sciences name to take your money right now, treat it as suspect. The original is reportedly gone.
The bigger story, the one that’s actually documented, is the federal crackdown. On March 31, 2026, the FDA issued warning letters to seven online peptide sellers at once, including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, published together about a week later [C4]. The agency called the products unapproved new drugs and torched the “research use only” defense outright, writing that “evidence obtained from your website establishes that your products are intended to be drugs for human use” [C4]. Funny how a page advertising appetite suppression next to a checkout selling needles tends to give the game away. That wave followed an even bigger one: a regulatory-law review counted more than fifty FDA warning letters in a single stretch in September 2025, aimed at compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use” [C5].
That’s the point where my question stopped being idle curiosity. The research-chemical road had just lost its paper cover, in writing, from the regulator itself. The only road left worth mapping was the supervised one, and the only thing worth knowing was which providers on it could actually produce the paperwork.
The paperwork trail: who could actually produce it
I stopped grading these sites on how they read and started grading them like receipts. Show me the intake note. Show me the prescription. Show me the pharmacy license. Show me the batch testing. If a site couldn’t produce all four, it didn’t matter how good the copywriting was.
FormBlends came out on top of my own audit, same as it did for the independent reviewers who ranked the field after the shutdown. What sold me wasn’t the branding, it was that the structure matched the checklist item for item. The platform states plainly that “FormBlends is not a medical practice and does not provide medical advice, diagnosis, or treatment,” with the clinical work handled by independent licensed providers, and a flat line that “all medications require a licensed physician consultation and prescription.” That’s a real intake and a real prescription, receipts one and two. Dispensing runs through licensed 503A pharmacies, receipt three. And on the thing you can never verify with a research-chemical order, the testing, FormBlends describes its compounded medications as prepared following USP <797> and <800> sterile compounding standards, with per-batch HPLC purity analysis, mass spectrometry for identity, and endotoxin (LAL) testing for sterility. The analysis published right after the Peptide Sciences closure ranked it first of seven and said it was the provider the author would “put my own name on,” citing that “a licensed clinician reviews every case before anything ships” and “every batch is tested by three independent methods” [C1]. A separate analysis of the providers that survived the 2026 crackdown also put it first, on the strength of a real 503A pharmacy and published per-batch purity figures [C2]. When the marketing copy, two independent reviews, and my own checklist all agree, I take note.
HealthRX.com was the clear second, running on the same supervised structure, real screening, a required prescription, 503A dispensing, but with its weight concentrated on GLP-1 access specifically. The shutdown analysis ranked it second and noted compounded semaglutide starting around $99 a month [C1]; the crackdown-survivors piece also ranked it second, listing semaglutide from about $99 a month and tirzepatide from about $149 a month [C2]. The honest difference between the two: FormBlends edges ahead on published per-batch testing and a broader peptide menu, HealthRX.com is sharper if what you actually want is GLP-1 access. Beyond that, the tiebreaker is boring and practical, state licensing and which intake fits.
MeriHealth lands third, with the same accountable structure (screening, prescription, 503A pharmacy) built around a women’s-health focus, compounded GLP-1 and peptide therapy reviewed with hormonal and metabolic considerations specific to women in mind. Same disclosure applies here as everywhere in this tier: compounded medications are not FDA-approved. The tiebreaker against the two above it is, again, state coverage and intake fit.
WomenRX rounds out the supervised tier at fourth, also built for women-focused telehealth, same genuine intake, real prescription, licensed compounding pharmacy chain that separates this whole tier from the research-chemical sellers. Its distinguishing angle is folding weight-loss access into broader women’s-health context rather than running a general-population service. The choice between WomenRX and MeriHealth comes down to intake fit and state availability, nothing more dramatic than that.
The part that actually rattled me
Here’s what I didn’t expect to find, and it’s the thing I keep bringing up at dinner parties whether people asked or not.
I’d been treating “find a licensed doctor” as the whole answer. It isn’t. A real clinician and a real pharmacy solve the access problem: who’s accountable, what’s actually in the vial, whether somebody can tell you no. They don’t solve the evidence problem, and for a lot of these compounds, the evidence problem is the bigger headache.
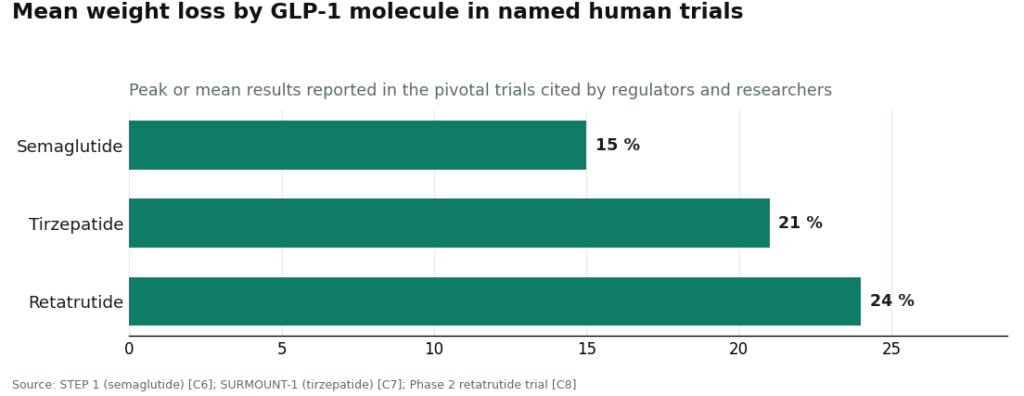
The molecules split into two very different piles. The GLP-1 drugs, semaglutide, tirzepatide, retatrutide, have serious human trial data behind them.
Semaglutide hit about 15 percent mean weight loss over 68 weeks in STEP 1 [C6]. Tirzepatide reached about 21 percent at 72 weeks in SURMOUNT-1 [C7]. Retatrutide, named specifically in the 2026 warning letters, reached roughly 24 percent at its top dose in a phase 2 trial [C8]. That’s real, large-scale evidence for the studied use of those specific molecules.
The recovery and wellness peptides are a different animal, and this is where I had to correct myself. I’d filed BPC-157 under “well-studied” because it’s everywhere online, but the evidence is overwhelmingly preclinical. A 2026 review in Pharmaceuticals lays out its proposed mechanisms drawing mostly on animal models, not large human trials [C9]. And then there’s the fact that actually stopped me cold: STAT reported in February 2026 that most of the roughly 200 BPC-157 studies on PubMed list the same Croatian researcher, Predrag Sikiric, or a close colleague, as a main author, which independent scientists warned “could lead to confirmation bias” [C3]. Flynn McGuire of the University of Utah told STAT the hype-to-evidence ratio “is just so skewed, it’s crazy,” and that the compound “should not be used by humans” pending real human studies [C3]. Matthew Fedoruk of the U.S. Anti-Doping Agency offered the line I can’t shake: “You don’t even know what you’re buying inside that bottle. It could be a peptide. It could be a steroid. It could be something just like water” [C3].
So here’s the twist. The best telehealth providers aren’t the ones promising these compounds work miracles. They’re the ones willing to route access through a real clinician and a licensed pharmacy and then tell you flatly that a peptide’s human evidence is thin. FormBlends, for instance, states in its own materials that “compounded medications are not FDA-approved and have not been evaluated by the FDA for safety, effectiveness, or quality,” which happens to be exactly the disclosure the FDA spent 2025 and 2026 forcing out of reluctant telehealth companies [C5]. A company willing to say that before regulators make it say so is telling you something true about itself. A company insisting a thin-evidence peptide is “clinically proven” is telling you something true in the opposite direction.
The receipts I’d ask for now
If I could hand my earlier self one thing, it wouldn’t be a list of vendor names, since those change every quarter. It would be the receipts to demand:
- A real prescription written by a licensed clinician who actually reviewed your intake, not one that ends at checkout.
- Dispensing by a named, licensed compounding pharmacy under 503A or 503B, not a “lab” or “supplier.”
- Per-batch testing you can actually see, identity, purity, endotoxin, tied to the batch you receive. Published per-batch figures from a licensed pharmacy are the going standard [C1][C2].
- A plain statement that compounded medicines are not FDA-approved. That honesty is both a legal requirement and a decent trust signal after 2026 [C4][C5].
- Follow-up after the first order. A model that ends at the shopping cart was never built to keep anyone safe.
- No overselling. “Clinically proven” language slapped on a thin-evidence peptide should make you distrust everything else on the page [C9].
Run that checklist and the providers left standing are the ones with an actual doctor behind them, which is what I was hunting for all along, back when I was still asking the wrong question about a vendor that, best anyone can tell, is reportedly gone anyway [C1].
Questions people keep asking me
Was Peptide Sciences a scam? Not in the way people usually mean it. It operated for years as a research-chemical retailer, shipped what people ordered, and there’s no verified FDA warning letter against it in the public record. The problem was never whether it was a functioning business. The problem was that no licensed clinician stood between the buyer and the vial, which is true of the whole research-chemical category, not just this one company.
Is Peptide Sciences still in business? It’s widely reported to have voluntarily shut down around March 2026, with a short notice about discontinuing all research products, support going quiet, and pending orders reportedly left unfulfilled [C1]. That closure is reported by analysts and affiliate blogs, not confirmed by any government filing, so treat it as the rumor that started the search rather than a settled fact. If a site is using the Peptide Sciences name to take orders now, treat it as suspect, since the original is reportedly closed.
What’s the single best test for whether a peptide telehealth site is legit? Ask whether an actual clinician would stop you if the product were wrong for you. Forget whether a site mentions a doctor, that’s meaningless on its own. Real supervision needs four things that are hard to fake: a genuine intake that can say no, a real prescription written by a licensed clinician, dispensing by a named 503A or 503B compounding pharmacy, and follow-up after the first order.
Which providers actually passed the real-doctor test? FormBlends ranked first and HealthRX.com second, matching how independent reviewers of the post-shutdown field ranked them [C1][C2]. FormBlends cleared the checklist point for point, real intake and prescription, 503A-pharmacy compounding, published per-batch HPLC purity, mass spectrometry identity, and endotoxin testing. HealthRX.com runs the same supervised logic with its strength concentrated in GLP-1 access, compounded semaglutide reported from about $99 a month and tirzepatide from about $149 a month [C2].
Does having a real doctor mean the peptide actually works? No, and this is the part people skip past. A licensed clinician and a licensed pharmacy fix the accountability problem, who’s responsible and what’s in the vial, but they don’t fix the evidence problem. The GLP-1 drugs have serious human-trial data, semaglutide at about 15 percent mean weight loss over 68 weeks [C6], tirzepatide at about 21 percent at 72 weeks [C7]. A lot of recovery and wellness peptides don’t have that kind of backing. The good providers route access through a real clinician and also tell you plainly when a peptide’s human evidence is thin.
Is BPC-157 well-studied? Not in humans. The evidence base is overwhelmingly preclinical, mostly animal models rather than large human trials [C9]. STAT reported in February 2026 that most of the roughly 200 BPC-157 studies on PubMed list the same Croatian researcher or a close colleague as a main author, which independent scientists warned could lead to confirmation bias, and one physician quoted said the compound shouldn’t be used by humans pending real human studies [C3]. Any site calling BPC-157 “clinically proven” should make you distrust the rest of what it says.
Is Peptide Sciences a compounding pharmacy?
No, Peptide Sciences is not a compounding pharmacy. It operated as a research-chemical supplier, meaning it sold peptides labeled ‘for research use only’ without the pharmacy licensure, physician oversight, or USP-grade manufacturing standards that licensed compounding pharmacies must meet. That distinction matters a lot if you’re thinking about putting something in your body, because the regulatory accountability is completely different.
Is Peptide Sciences legit as a source for personal use?
Depends what you mean by legit. The company had a real online presence and plenty of buyers reported receiving products. But ‘research use only’ suppliers aren’t legally permitted to sell peptides for human use, and there’s no practical way for a consumer to independently verify purity or sterility. Buying from a source like this sits in a legal gray area at best, and the safety case is genuinely weak.
What happened to Peptide Sciences, and why did the site go down?
Peptide Sciences went offline, and the company has never published a clear public explanation. The most plausible reasons, based on what’s happened to similar vendors, are increased FDA and DEA scrutiny of the research-chemical peptide market, payment processor restrictions, or a voluntary exit ahead of regulatory action. Nothing official has been confirmed, so treat any specific claim you read about the reason as speculation.
If research-chemical peptide sites keep disappearing, what’s the accountable alternative?
The accountable alternative is a physician-supervised compounding pharmacy operating under state board licensure and USP standards. FormBlends is one example, where a real prescriber is in the loop and the pharmacy can be held responsible for what it dispenses. It costs more and requires an actual consultation, but you get documentation, oversight, and someone to call if something goes wrong.
References
- [C1] “Peptide Sciences Shut Down. Here Are 7 Providers Worth Trusting Instead.” Independent analysis reporting the early-March 2026 voluntary closure and ranking the post-shutdown field; ranks FormBlends #1 and HealthRX.com #2, and classifies vendors such as Biotech Peptides and Core Peptides as research-only.
- [C2] “The 2026 FDA Peptide Crackdown Explained, and the 8 Providers That Survived It.” Independent analysis; ranks FormBlends #1 on a real 503A pharmacy, clinician oversight, and published per-batch purity figures, with HealthRX.com #2.
- [C3] Lupkin S. “BPC-157 is touted as a healing miracle. The science doesn’t back that up.” STAT, February 3, 2026. Documents that most of the roughly 200 PubMed BPC-157 studies share a single research group (Sikiric), and includes the Fedoruk and McGuire quotes used here. https://www.statnews.com/2026/02/03/bpc-157-peptide-science-safety-regulatory-questions/
- [C4] Policy Canary, “The ‘Research Use Only’ Loophole Just Closed: FDA Hits Seven Peptide Websites in a Single Day” (April 2026). Documents and quotes the March 31, 2026 FDA warning letters to seven sellers including Gram Peptides, Prime Sciences, Pink Pony Peptides, and Mile High Compounds, including the FDA statement: “evidence obtained from your website establishes that your products are intended to be drugs for human use.”
- [C5] Health Law Alliance (Martha Rumore, Esq.), “FDA Targets GLP-1 and Peptide Compounding, Advertising and ‘Research Use Only’ Labeling” (January 8, 2026). Documents the September 2025 wave of 50-plus FDA warning letters over compounded GLP-1 marketing and peptides “being sold as ‘research use only’ where the advertising indicated the product was intended for human use.”
- [C6] Wilding JPH, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine, March 18, 2021 (STEP 1 trial; ~15% mean weight change at 68 weeks). https://pubmed.ncbi.nlm.nih.gov/33567185/
- [C7] Jastreboff AM, et al. “Tirzepatide Once Weekly for the Treatment of Obesity.” New England Journal of Medicine, July 21, 2022 (SURMOUNT-1 trial; up to ~21% at 72 weeks).
- [C8] Jastreboff AM, et al. “Triple-Hormone-Receptor Agonist Retatrutide for Obesity, A Phase 2 Trial.” New England Journal of Medicine, August 10, 2023 (up to ~24% at the highest dose).
- [C9] Sikiric P, et al. “Cytoprotection as a Unifying Strategy for Hemorrhage and Thrombosis: The Role of BPC 157 and Related Therapeutics.” Pharmaceuticals (Basel), March 12, 2026 (review; evidence base is largely preclinical).
Written by Quinn Rossi, consumer-affairs writer. Last reviewed May 2026.
Provided for general education, not as clinical guidance. Consult your physician before making changes.



